What do You Know About Autism?
Estimated reading time: 5 min
Target audience: Laypeople - No prior knowledge necessary
A bit more than a year ago, I was interviewed for an article in one of the largest daily newspapers in Serbia (Politika) titled “Autism does not only affect males”. The goal was to add to the growing literature in the public domain that aims to educate laypeople about neurodevelopmental disorders in general, and autism specifically. To the detriment of patients and their families, the current understanding among laypeople is still far behind that of the medical profession, even in Sweden. In Serbia, this understanding is not even measured on the same scale…
I was naive to think that the topic of female autism would be ripe in Serbia, when it is barely that in Sweden. Knowledge is cumulative, and one can sometimes outline a general pathway from ignorance to understanding. I will briefly outline such a pathway for autism below, which may help identify at which level one should focus one’s intentions to reap the greatest benefits of a public discourse surrounding autism. In a later blog post, I will expand on the topic of female autism, and translate parts of the text from the above-mentioned article.
Since autism was first described, the general understanding of this condition has undergone major changes in a relatively short time. Only decades ago, it was still believed that the behavior of the mother was a cause of autism. The origin of the idea of the “refrigerator mother”, despite being completely wrong, has an explanation: mothers with autistic-like traits exhibit more behaviours that may derogatorily be described as refrigerator-like, and their children inherit those traits, giving them a higher likelihood of receiving a diagnosis. Without an understanding of heredity, this was an easy mistake to make.
Since then, the understanding of autism has vastly expanded, and we now know that:
It is highly hereditary. Genetic studies show that it is one of the most hereditary conditions within psychiatry.
It is present at birth. Many studies have identified differences in behaviour already in the first months of life and with improved methods these differences keep being identified earlier and earlier. Recently, a pretty cool study showed that babies, already before birth, prefer viewing “faces”, and since this preference has been shown to differ in babies with autism after birth, it is likely that a similar study would identify prenatal differences in those that later develop autism.
It is life-long. Although the symptoms can get better over time, with some individuals even losing the diagnostic label, there is no indication that autism can be “cured”.
Environmental factors have been shown to increase the risk; particularly pregnancy-related complications in individuals with a genetic predisposition. The risk factors are biological in nature. Behavioural factors, such as targeted training of social skills, can lower the disability associated with autism; similarly, lack of such training can increase the level of disability. However, there are no indications that any behavioural factors, such as prolonged screen time, can cause autism. It is worth mentioning that infections during pregnancy, such as rubella, have been associated with an increased risk of autism. For this reason, some studies have actually associated non-vaccination with autism, and this is the only rational and evidence-based connection between vaccines and autism to date. More on this pressing topic in another post.
The traits and symptoms associated with autism exist in the general population. Autistic-like traits are normally distributed in the population, and it seems that autism merely represents the upper end of that spectrum (hence one of the interpretations of the name “autism spectrum disorders”). These traits are particularly frequent in relatives of individuals with autism, for obvious reasons, where they are referred to as the “broader autism phenotype”. These traits confer multiple surprising strengths. They are the topic of my Bachelor thesis in psychology, and I will devote a later blogpost to this.
There are many behavioural presentations of autism, and it appears to be particularly different in females. In individuals with normal IQ, there is a large discrepancy between the number of males and females being diagnosed. Females with a diagnosis generally have a higher disease burden than males, which has been attributed to some protective effect in females. One possible reason is that females in general have a higher social intelligence and greater propensity for communication and fitting in, which may cause female autism to go unrecognised. Despite having greater social abilities, the core deficits remain, leading many to unsuccessfully undergo treatment for misdiagnosed social phobia, anxiety, and anorexia. As such, there is a pressing need for more targeted studies on female patient populations and development of biologically rooted diagnostic tests (one of the main aims of my PhD).
Naturally, one focuses one’s effort on solving the greatest problems first, only later becoming interested in more nuanced issues. Before understanding what autism is and what causes it, it would be inefficient to investigate why more males than females are affected. Obviously, an understanding of what autism is and being able to correctly identify it are the bare minimum for any discussion. Understanding that it is largely biologically determined (inherited and a result of biological insults) is a prerequisite for further studies and rational discussions surrounding it. Only then can one begin to discuss specific causes, followed by an understanding that there is a continuous distribution of such traits in the population, that the female presentation differs compared to males, and finally that there are strengths associated with autism and autistic-like traits, which are likely the reason why natural selection has not eliminated them.
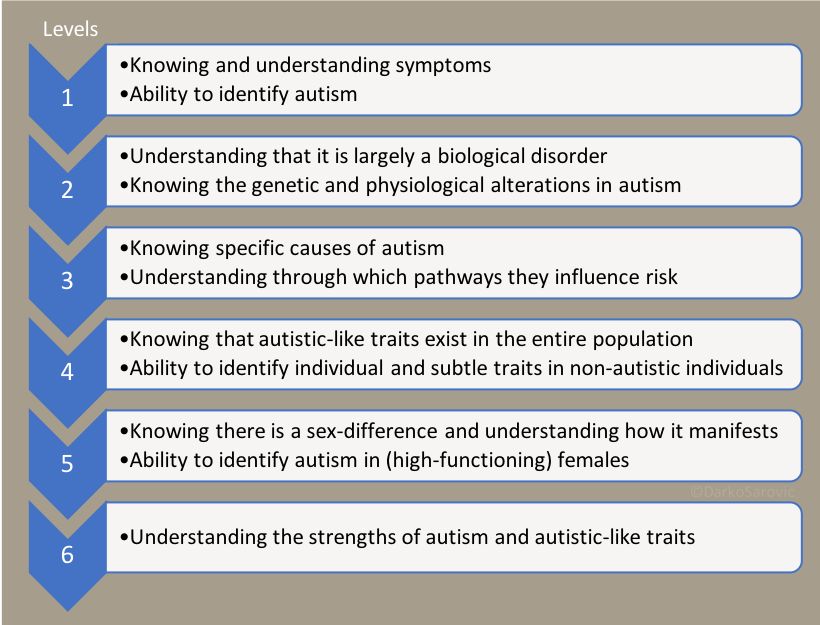
A pathway toward understanding autism. Each level represents a less pressing and more nuanced understanding. Also, each level is a prerequisite for understanding and discussing higher levels. If someone is not aware that autism is biologically rooted, it is fruitless to discuss specific causes. Similarly, before someone knows what autism is and its symptoms, any discussion will be muddled by misunderstandings and mixups with other conditions.
Before attempting any educational measures, one needs to identify at which level the current understanding is. In Serbia, the general understanding of autism is still entirely constricted to the neuropsychiatric subspecialists, while that of Sweden has largely spread to other specialties, such as paediatricians and general practitioners, which are now able to correctly identify and refer suspect cases for an evaluation. Due to the lack of explanations for why and how females with autism differ from males, Sweden now faces the issue of identifying females with autism for referral to a neuropsychiatrist.
The take home message from this idea is that one must first determine the target audience of the educational measure, identify their level of understanding, and only then implement educational measures. Until the general public in Serbia understands that autism is biologically determined, it is largely useless to discuss male-female differences or specific causative factors.
I urge you to think about your own understanding of autism:
At which level is your own current understanding?
What information are you missing in order to gain an increased understanding?
What are the steps you can take toward achieving the next level?
Feel free to write your conclusions (and comments on the text) in the comments-section below, and perhaps we can identify knowledge gaps and possible pathways to fill those gaps (and thus topics for future posts).